

Reducing Male Extrusions and the T100 Protocol
Pellet therapy delivers consistent bioidentical testosterone in a physiologic manner for men and has many advantages over injections, gels, creams or troches.i,ii,iii However, one disadvantage is the number of pellets needed and the subsequent development of scar tissue–resulting in a higher risk of pellet extrusionsiv.
This can be improved by changing the area of delivery from the gluteal area to the flank or abdomen. In addition, one could opt to utilize an outside-in approach from lateral to medial after several years of normal inside-out placement of pellets in the flank.
Another option introduced by Drs. David Watson and Bruce Dorr (Denver, CO) in 2019 is the T100 Technique for males, which uses T100 pellets in place of the T200 pellets. This approach has been shown to have many advantages. The incision is smaller and the blade of the T100 trocar tends to be sharper and smaller, making it advance through the tissue easier and result in less scarring. Rather than 4 pellets in each track, the smaller pellets allow up to 6 in each track—directing the insertions at the 2, 4, 6 o’clock, etc. positions. The importance of maintaining the hub of the trocar against the skin with each pellet delivery remains vital as it minimizes distal tip movement and tissue damage. As a result, the T100s tend to not be extruded as often as the T200 pellets, perhaps due to size of the track created to place them.
The uptake of testosterone is based on the surface area of the pellet. After insertion, the body surrounds the pellet with a capillary network, then cardiac output drives the delivery of testosterone into the bloodstream—which is physiologically similar to the testicles. The surface area difference between two T100 pellets and one T200 pellet is approximately 30%. It is important to note that the clinical decision support software will decrease the dose by approximately 40%, as the 30% calculation resulted in elevated levels of testosterone in the initial studies.
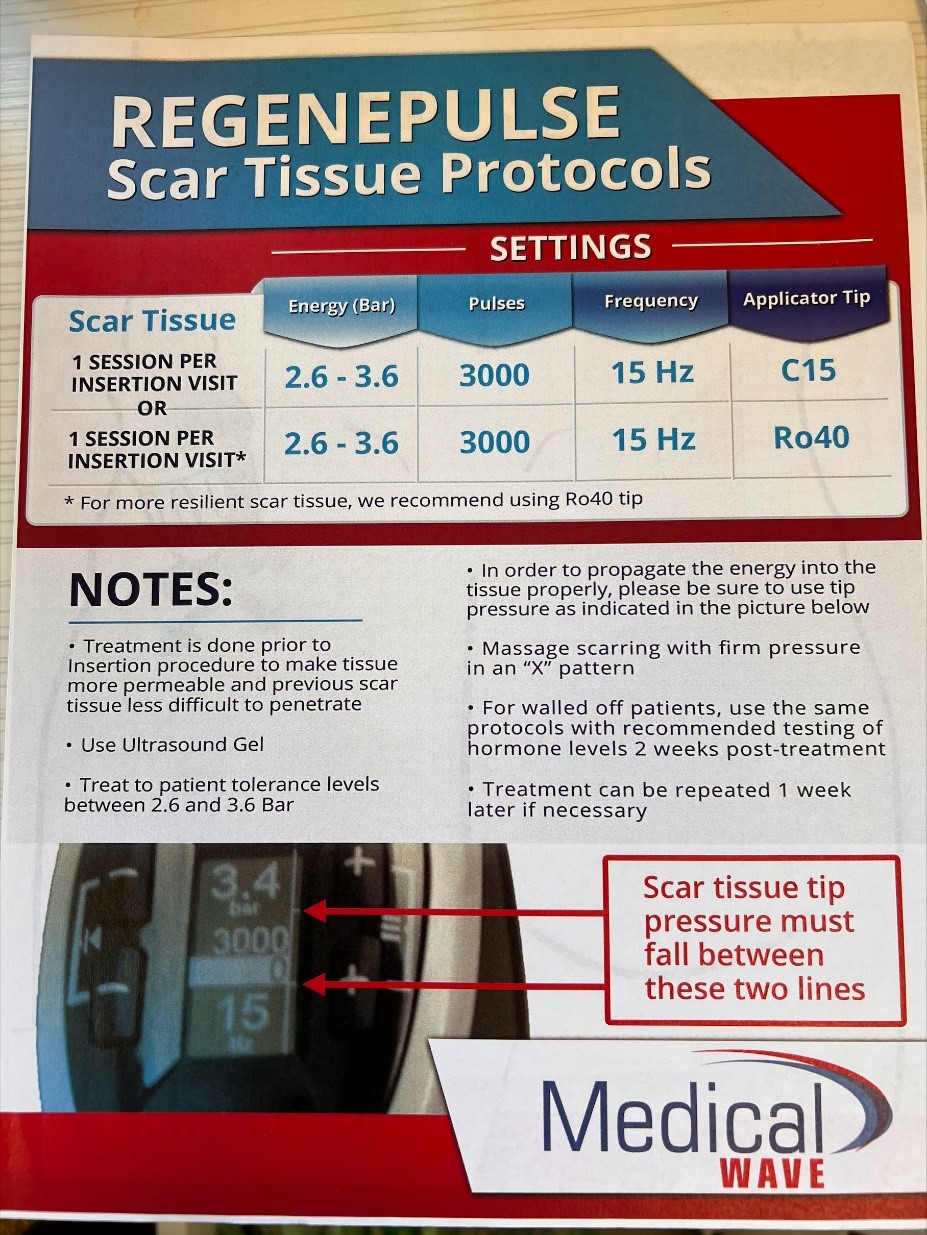
Another method to decrease scar tissue is utilizing extracorporeal shockwave therapy (ECSWT). ECSWT has been shown to increase blood flow, promote healing and break up scar tissue throughout the body. It is used to effectively treat tendinitis, fasciitis and musculoskeletal pain for decades. By using a shockwave therapy at the area of previous pelleting, it can promote revascularization and prevent scar tissue development to allow continued pelleting in the same area. Be aware that device settings may vary between the 2 major manufacturers, Storz and Zimmer—see Figure 1 and refer to the manufacturer’s instructions for use.
Lastly, adding 1/2 cc of a water-soluble steroid, betamethasone/Celestone® (6 mg/ml vial), is an excellent option to decrease inflammation in scarred or extrusion prone patients. This is typically mixed with the lidocaine anesthetic and injected prior to pellet insertion.
Figure 1
- Greenblatt RB, Suran RR. Indications for hormonal pellets in the therapy of endocrine and gynecic disorders. Am J Obstet Gyncol. 1949; 57:249-301.
- Thom MH, Collins WP, Studd JW. Hormonal profiles in postmenopausal women after therapy with subcutaneous implants. Br J Obstet Gynaecol. 1981 Apr;88(4):426-33.
- Stanczyk FZ, Shoupe D, Nunez V, Macias-Gonzales P, Vijod MA, Lobo RA. A randomized comparison of nonoral estradiol delivery in postmenopausal women. Am J Obstet Gynecol. 1988 Dec;159(6):1540-6.
- Donovitz GS. Low complication rates of testosterone and estradiol implants for androgen and estrogen replacement therapy in over 1 million procedures. Ther Adv Endocrinol Metab. 2021 May 27; 12: 1-11